Paraesophageal Hernia
What is a paraesophageal hernia?
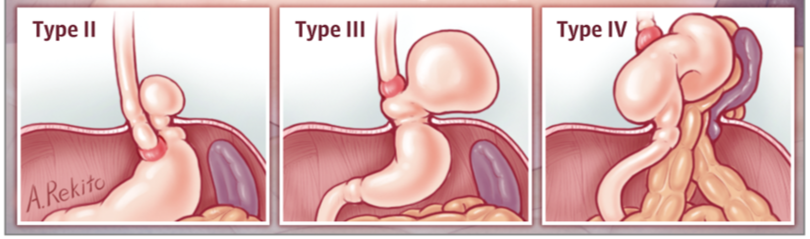
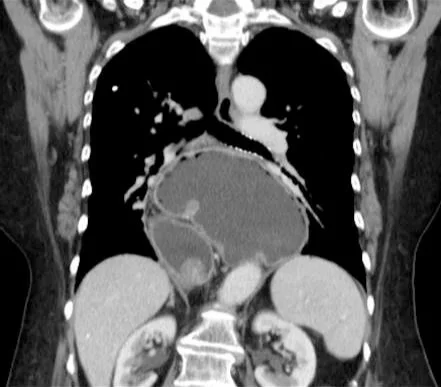
A paraesophageal hernia occurs when there is an opening in the diaphragm that allows some or all of the stomach to move up into the chest cavity behind the heart.
When should a paraesophageal hernia be repaired?
In general, all paraesophageal hernias causing symptoms should be repaired. Common symptoms from a paraesophageal hernia include:
Chest pain—there are many causes for chest pain. It is important that patients who have a large paraesophageal hernia with chest pain undergo some kind of a cardiac evaluation to make sure that the chest pain is not from their heart. Typically, eating brings on chest pain from a paraesophageal hernia. Some patients have pain every time they eat, and others only experience discomfort every once in a while.
Epigastric pain—this is pain in the middle, upper abdomen.
Dysphagia—difficulty swallowing.
Shortness of breath—in some very large paraesophageal hernias, the stomach may push on the diaphragm or compress the lungs contributing to a sensation of shortness of breath. There are many other reasons for shortness of breath in addition to a paraesophageal hernia.
Early or prolonged satiety—Because the stomach is twisted or compressed due to the hernia, it may be difficult for patients to eat a normal sized meal. Patients may feel full for a very long time after eating, which is due to the fact that the stomach can’t empty normally when it is herniated. Some patients may lose weight because of difficulty eating.
Stomach ulcer—in some patients with paraesophageal hernias, the stomach may twist upon itself resulting in a specific kind of stomach ulcer known as a Cameron’s erosion. These ulcers can occasionally contribute to chronic slow blood loss and anemia.
Stomach volvulus: A rare complication but serious and life-threatening complication of a paraesophageal hernia is when the stomach twists on itself, blocking the blood flow and passage of food, liquids and secretions. This is called a stomach (gastric) volvulus and can lead to a rupture of the stomach, sepsis and death if not treated with emergency surgery.
Many patients (but not all) with paraesophageal hernias may also suffer from gastroesophageal reflux disease symptoms. GERD by itself is not a reason to repair a paraesophageal hernia. GERD is first treated with medications, and surgery is reserved for those who fail medical management.
How are paraesophageal hernias repaired?
Almost all paraesophageal hernias can successfully and safely be repaired laparoscopically (with about 5 very small incisions) and through the abdomen (rather than the chest cavity). The laparoscopic repair of large paraesophageal hernias (most of the stomach resides above the diaphragm in the chest cavity) is a complex procedure and should only be attempted by expert laparoscopic surgeons with extensive experience in laparoscopic foregut surgery.
During surgery, the large hernia sac that holds the stomach up in the chest is carefully dissected away from the aorta, lungs and spine which allows the stomach to be brought back into the abdominal cavity without tension. The diaphragm at the esophageal hiatus is closed to prevent the stomach from re-herniating. Sometimes a counter incision is needed in the diaphragm to reduce tension on the closure. In addition, we use pledgets to add strength to the repair of the muscle and a reinforcing absorbable or biologic mesh is use to ad strength to the repair. Once the diaphragm has been closed, most patients undergo a fundoplication or a ‘wrap’ similar to what is done for a patient with GERD. The fundoplication is performed to help keep the stomach from herniating back into the chest cavity.
What are the results of paraesophageal hernia repair?
When performed by experienced surgeons who specialize in esophageal surgery, the results of robotic paraesophageal hernia repair are excellent. This minimally invasive approach results in significantly fewer complications and most patients are only in the hospital overnight and are back to their usual activities within 4 weeks.
Side effects can occur and are similar to those observed after laparoscopic Nissen fundoplication. Abdominal bloating can occur but is rarely severe. Difficulty swallowing (dysphagia) is another side effect that tends to improve in most patients with time. The majority of patients are able to belch easily when necessary; especially once some time has passed following surgery.