What is achalasia?
Achalasia is a rare esophageal disorder that develops when your esophagus doesn’t move food and liquid to your stomach like it should.
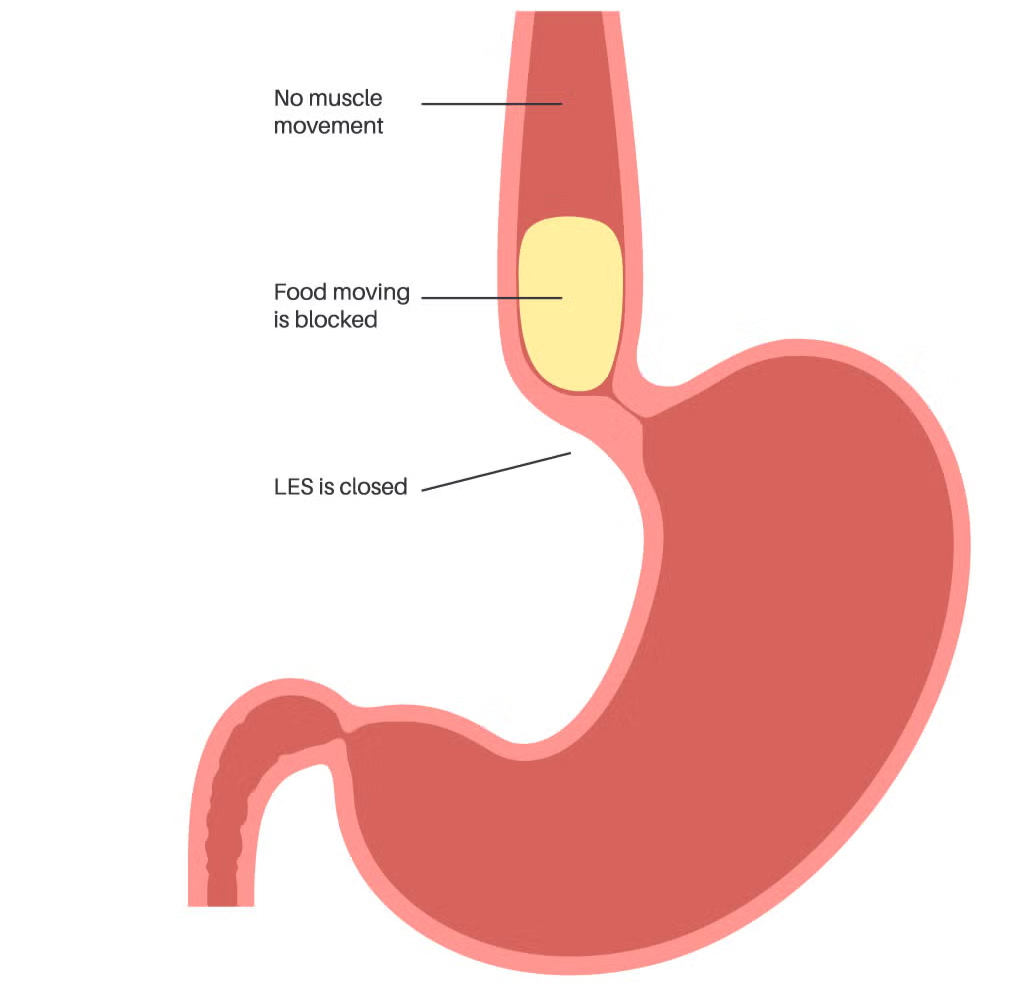
Your esophagus is a muscular tube that runs from your mouth to your stomach. Normally, muscular contractions in your esophagus push food and liquid down to your lower esophageal sphincter (LES). Your LES is a ring-shaped muscle that relaxes (opens) to let food move into your stomach and tightens (contracts) to keep contents in your stomach from backing up into your esophagus.
In achalasia, the normal esophageal muscular contractions do not take place or do not work as well as they should. In addition, the LES doesn’t relax, so what you eat and drink stays in your esophagus instead of moving into your stomach.
Esophageal Motility Disorders
What are the symptoms of achalasia?
Achalasia symptoms develop slowly. You can have this disorder for months or years before noticing changes in your body. Symptoms include:
Difficulty swallowing or the feeling like liquid and solid food is stuck in the esophagus and not emptying into the stomach
Bringing swallowed food back into your mouth
Chest pain, spasms that comes and goes and may be severe
Heartburn
Hiccups
Unexplained weight loss
What causes achalasia?
We don’t know the exact reason why your esophagus doesn’t work like it should. One theory is that achalasia is an autoimmune disease (your body attacks itself) that a virus triggers. In this theory:
Your immune system attacks the esophagus where the nerves connect to the muscle.
Under attack, these cells slowly deteriorate.
They stop driving the process that moves food and liquid through your esophagus to your stomach.
What are the complications of achalasia?
If you have achalasia, food may back up into your esophagus and into your windpipe, so you inhale food into your lungs. If that happens, you may develop complications like:
Aspiration pneumonia
Lung infections
Malnutrition
How do we diagnose achalasia?
Dr Reising and his team will do a take a thorough history and exam. They’ll ask you to describe your symptoms and how long you’ve had them. We do three tests to diagnose achalasia:
Esophagram test (barium swallow)
Esophageal manometry test
Upper endoscopy
How is achalasia treated?
Treatment focuses on relaxing your LES, the ring of muscle at the base of your esophagus. Treatment can’t cure achalasia, but nonsurgical and surgical options can help ease symptoms. Your healthcare provider will plan treatment depending on factors like your symptoms and your personal preferences. They’ll discuss these options with you so you both can decide what treatment makes sense for you.
Nonsurgical treatment for achalasia
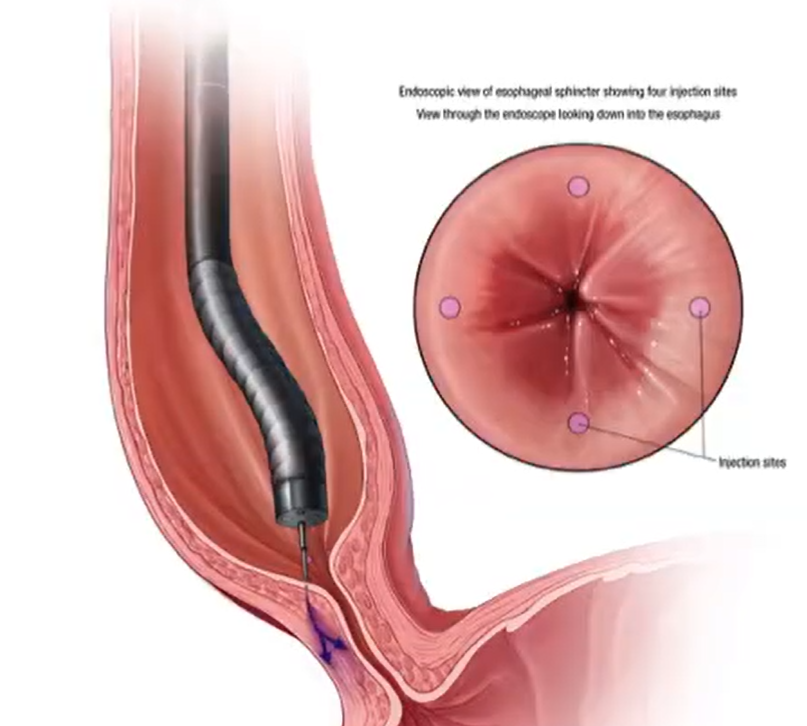
Medication. This is another way to loosen your LES. Your provider may recommend injecting Botox into your LES. I don’t recommend Botox because it makes future surgical treatment more difficult and riskier. Other options include nitroglycerin and calcium channel blockers. Results are not very good with medications.
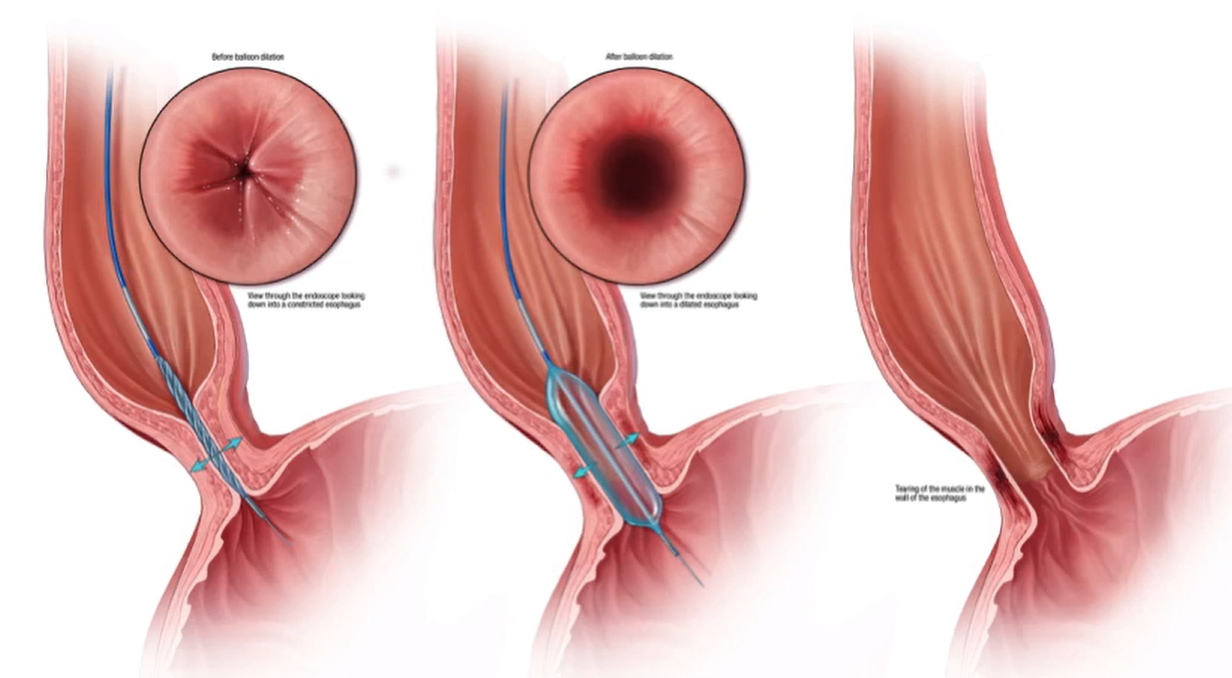
Balloon dilation. This procedure involves inserting a specifically designed balloon through your LES. You’ll be under anesthesia during the procedure. Your provider inflates the balloon, which helps the muscle relax so food can move to your stomach. You may need several treatments to relieve your symptoms.
Surgical treatment for achalasia
Dr. Reising may recommend one of two minimally invasive surgeries to loosen your lower esophageal sphincter (LES). Those surgeries are:
Robotic Heller myotomy. Dr. Reising performs this surgery while you are asleep with several small fingertip sized incisions on your abdomen and cut the tight muscle on the upper stomach and lower esophagus where the lower esophageal sphincter is located. Most patients stay overnight and then are discharged home the next morning.
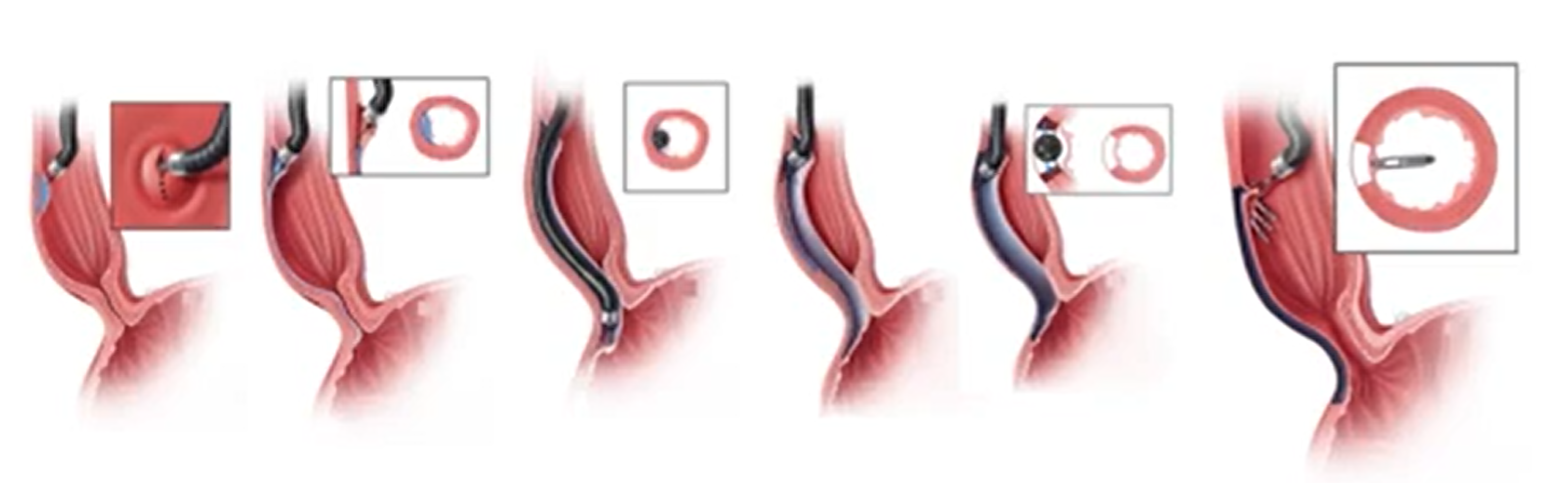
Peroral endoscopic myotomy (POEM). Dr. Reising does this procedure with you under anesthesia using an endoscope passed through the mouth and into the esophagus. The lining of the esophagus is cut with a special knife and the scope is carefully passed between the layers of the esophagus lining and the muscle all the way to the upper stomach. Once the tunnel has been created the tight muscle is divided with the knife and then the tunnel is closed with clips. Typically, you stay overnight in the hospital and then go home the next morning after a swallow test is performed.
Very rarely, your symptoms may be so severe that your provider will recommend an esophagectomy to remove your esophagus.
Treatment outcomes and potential complications
Dr Reising has excellent outcomes with both robotic Heller myotomy and POEM surgery. Both are safe and highly effective, in fact you will notice an immediate improvement in most cases right after surgery. Potential complications from these procedures include: complications:
Achalasia symptoms that come back which is usually a sign of an incomplete myotomy
GERD, which can happen in about 15-20% of patients and require and antacid medication
Esophageal injury leading to a serious infection. Thankfully, Dr. Reising has never had this complication even after treating hundreds of patients with achalasia over the last 26 years.