Gastroparesis
New!What is Gastroparesis?
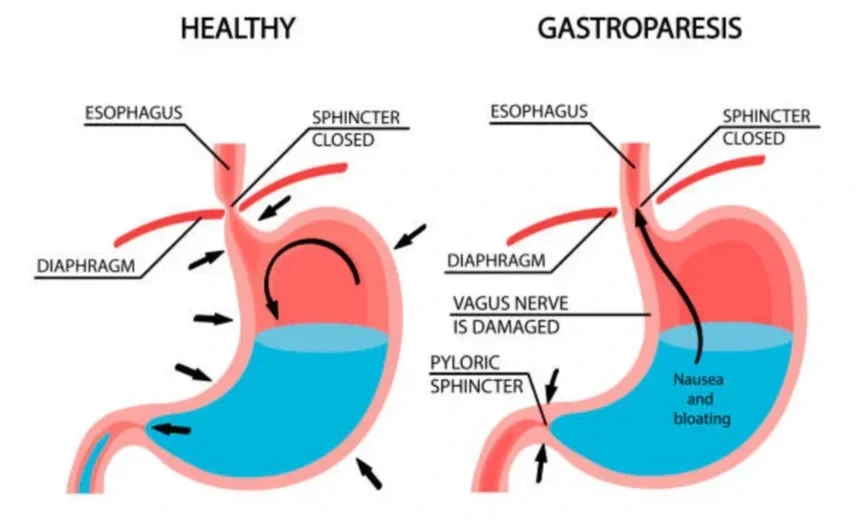
Gastroparesis is a condition where the stomach muscles don't work properly, slowing down or stopping the movement of food. It can be caused by:
Diabetes
Post-surgical nerve damage
Medications
Unknown reasons (idiopathic)
Common symptoms include:
Nausea and vomiting
Feeling full quickly when eating
Bloating or upper abdominal discomfort
Poor appetite and weight loss
How is Gastroparesis Treated?
Treat underlying or contributing causes
Improve control of chronic conditions (e.g., diabetes).
Review and stop medications that slow gastric emptying if possible (opioids, certain antidepressants, calcium channel blockers, anticholinergics).
Treat autoimmune, infectious, or metabolic causes when identified.
Lifestyle and dietary measures:
Eat smaller, more frequent meals (4–6 per day).
Choose low-fat, low-fiber foods that are easier to digest.
Favor liquids and pureed foods if solid foods are poorly tolerated.
Chew food thoroughly.
Sit upright for 1–2 hours after eating and consider light physical activity after meals.
For severe cases, consider nutrition support (enteral feeding via jejunostomy) or, rarely, parenteral nutrition.
Medications:
Some medication (called prokinetics) may to improve gastric emptying:
Metoclopramide: dopamine antagonist; can reduce nausea and improve motility. Risk of tardive dyskinesia with long-term use—use lowest effective dose and monitor.
Domperidone (where available): similar benefit with lower central nervous system side effects; may require special access in some regions.
Erythromycin (low-dose, short-term): motilin receptor agonist; effectiveness may wane due to tachyphylaxis.
Antiemetics for nausea and vomiting (ondansetron, promethazine, prochlorperazine) as needed for symptom control.
Glycemic control in diabetic gastroparesis: optimize blood glucose to improve symptoms and gastric emptying.
Endoscopic therapies
Endoscopic balloon dilation of the pylorus: occasionally used in selected cases.
Botulinum toxin injection into the pylorus: temporary benefit for some patients; evidence is mixed and effects are often short-lived.
Gastric peroral endoscopic pyloromyotomy (G-POEM): endoscopic cutting of the pyloric muscle to improve emptying; considered for refractory gastroparesis, with growing evidence of benefit in selected patients.
Why is G-POEM recommended?
G-POEM is recommended when:
Medications and dietary changes haven’t worked
You have moderate to severe symptoms affecting quality of life
Tests (such as gastric emptying studies) confirm delayed stomach emptying
It’s a less invasive option than traditional surgery and can provide long-term symptom relief.
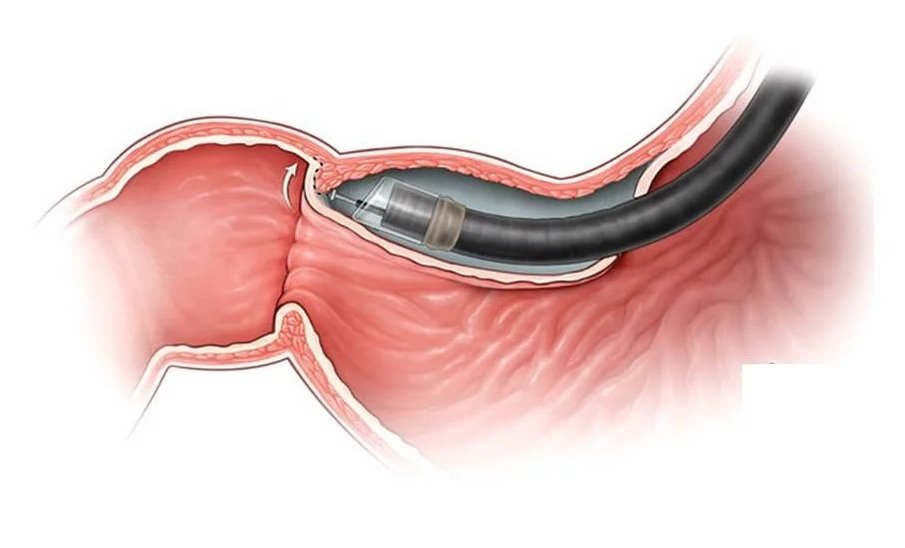
How is the procedure performed?
The procedure is done under general anaesthesia.
A flexible tube (gastroscope) is passed through your mouth into the stomach.
A tunnel is made under the stomach lining to reach the pyloric muscle.
The muscle is cut (myotomy) to allow food to pass more easily.
The tunnel is closed with small clips, which fall off on their own.
There are no external cuts or scars.
What are the benefits?
Minimally invasive
Improves stomach emptying
Reduces symptoms like nausea, vomiting, and bloating
Shorter recovery compared to traditional surgery
May reduce the need for long-term medications or feeding tubes
What are the risks?
While G-POEM is generally safe, possible risks include:
Bleeding: Usually minor and controlled during the procedure
Perforation: Rare, may require additional treatment or surgery
Infection: Antibiotics are given to reduce this risk
Reflux or indigestion: May occur after the procedure
No symptom improvement: In some cases, symptoms may persist or return
What happens after the procedure?
Most patients stay in hospital for 1 day.
You’ll start on clear fluids, then move to a soft diet, and eventually return to normal food over 1–2 weeks.
You’ll be monitored for complications and to ensure your stomach is emptying better.
Long-term care and follow-up
You’ll have regular follow-up with your doctor.
Some patients may need repeat testing or further treatment.
You may still need dietary advice or medications depending on your symptoms.
Frequently Asked Questions
Q: Will G-POEM cure gastroparesis?
A: It does not cure the underlying condition but can greatly improve symptoms in many patients.
Q: Is the procedure painful?
A: No, it is done under general anesthesia. Mild bloating or discomfort may be felt afterwards.
Q: How successful is G-POEM?
A: Studies show up to 60% symptom improvement.
Q: Can I eat normally afterward?
A: You’ll follow a special diet for a few weeks, gradually returning to normal eating.
Surgical interventions
Pyloroplasty or pyloromyotomy (open or laparoscopic): surgical widening or cutting of the pylorus to facilitate gastric emptying; considered when other treatments fail.
Gastric electrical stimulation (implantable gastric pacemaker): may reduce nausea and vomiting in refractory cases, particularly diabetic gastroparesis; benefit for emptying is variable.
Feeding jejunostomy or gastrostomy with jejunal extension for long-term enteral nutrition when oral intake is insufficient.
Enterra Therapy